
When you hear the word mobility what do you think of?
Do you think of foam rolling, lacrosse balls, bands, and a whole slew of other ways to “stretch out”?
When you hear mobility does the word flexibility come to mind as well?
In the fitness and healthcare industry, mobility and flexibility are often used synonymously, and although they are related, they are in fact completely different concepts.
Flexibility
Flexibility refers to the PASSIVE range to which the tissues surrounding a joint can move. It is the ability to achieve a range of motion with the assistance of other devices (i.e. a practitioner, a band, a wall). It allows you to see how compliant the tissues are and how well they stretch. Although flexibility has been seen as an important concept to address to decrease injury, the research actually shows that flexibility in itself is a very poor indicator of injury risk. Motor control of a joint is actually much more important at decreasing the risk of injury.
Mobility
This is where mobility comes in. Mobility refers to the ACTIVE range to which an individual can control their joint. It utilizes the components of flexibility (i.e., the tissue’s ability to stretch), as well as neurological control and strength. Mobility is created through progressive loading of a joint in different positions, much like the progressive loading done in strength training. This means that mobility must be trained actively, and cannot be achieved through simple static stretching and lacrosse ball “smashing”.
Check out this example below to understand the difference between flexibility and mobility:
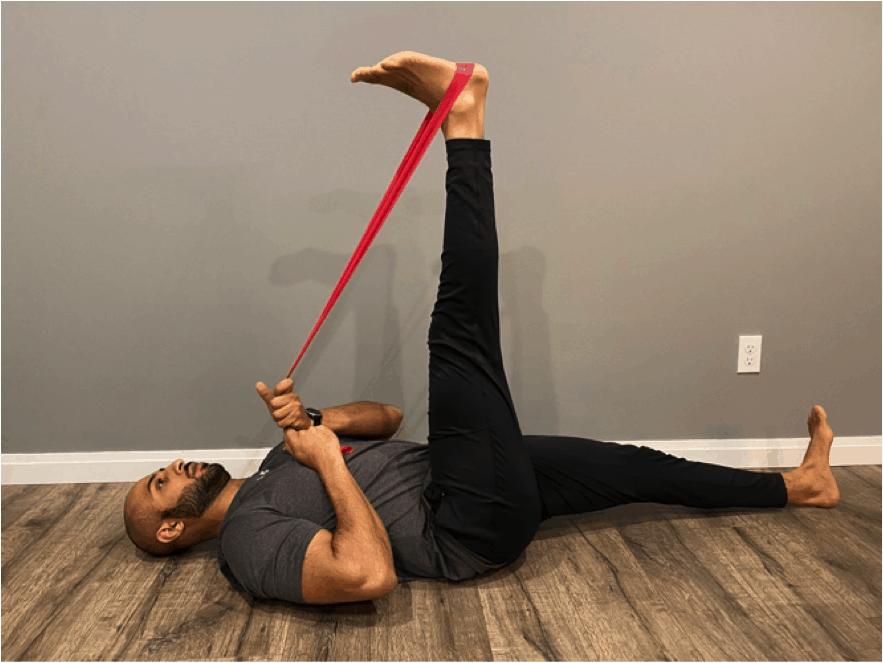
A) In the first picture, a band is used to achieve a stretch through the hamstring and move the hip into flexion. This would be the flexibility of the muscles on the back of the hip and knee allowing me to move into this position.
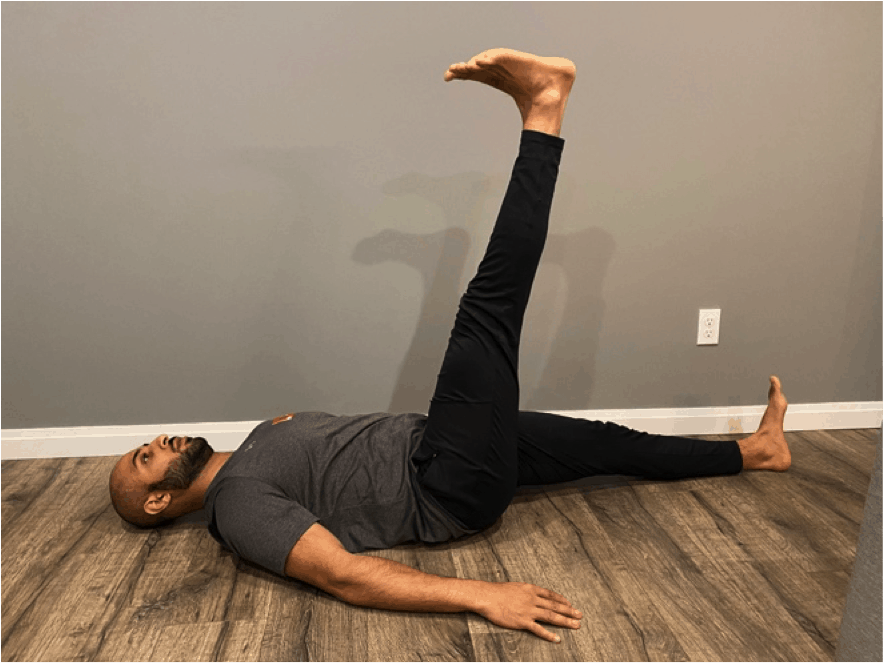
B) In the second picture, an ACTIVE straight leg raise is being performed. This uses the neurological control and strength of muscles on the front of the hip (hip flexors) and muscles that cross the knee (knee extensors), along with the flexibility of muscles on the back of the hip and knee.
What do you notice? This is a very common occurrence – most people have more ability to passively stretch into a position and less of an ability to actively control a joint into the same position.
This is extremely important because it opens the door to understanding why injury can occur. Most injuries occur due to an applied load that is greater than the capacity of the tissues being loaded. If our joint gets put into a position where we cannot actively control it, we cannot possibly protect it from external applied loads. In addition, without the appropriate motor control of a specific joint, how can we ask ourselves to perform more complex tasks, such as a squat? If the hip cannot actively move to the position that is needed in order to have a good squat pattern, then compensation is bound to occur at another area in the body (especially at the level of the knee, pelvis and low back).
If you’ve ever had low back pain or knee pain, has your practitioner ever assessed your hip to determine if it has the right motor control and mobility to be an active participant in more advanced movements?
Mobility training looks to improve isolated joint control and end-range strength before the joint is asked to integrate into a movement pattern. It works to prepare a joint for the inevitable variability it is to face when performing skills repetitively, as no one skill is ever performed with the exact same mechanics. By training the joint to it’s maximum capabilities, we are preparing the joint to be a functioning part of the whole. Isolate, then integrate.
If you have questions regarding mobility training and how it can be a great adjunct to improve your strength training along with mitigating your injury risk, ask a trusted rehab specialist.
Written by: Dr. Danny (Dhanbir) Dulay, Chiropractor